
Episode 122: AML Series, Pt 8 - AML Maintenance Therapies
This episode is sponsored by our Global Research Partners! Click here to get paid to participate in market research surveys!
What is the evidence for cytarabine consolidation?
Check out Episode 120 for much more detail!
For patients treated with intensive 7+3 induction chemo, studies in the late 1970s and 1980s including the ECOG E3483 and German AML group showed that patients that received no consolidation cytarabine had 100% relapse rates and poor overall survival
Randomized trials in the 1990s and 2000s including a 1994 CALGB study, CALGB 9222, and the AML2003 study showed that high dose cytarabine at 3 g/m2 on days 1, 3, and 5 every 28 days x 3 cycles was the optimal consolidation regimen
It was also shown that patients with a suitable donor should proceed directly to allogeneic transplant regardless of the number of consolidation cycles received
Patients older than 60 years of age have difficulty tolerating higher doses of cytarabine (3 g/m2) and studies such as the AML15 trial showed the feasibility of using 1.5 g/m2 on days 1, 2, 3 with G-CSF support with less toxicity
One network meta analysis showed with a weak level of evidence that lower doses may lead to inferior relapse-free survival, while the aforementioned AML15 trial showed a non-statistically significant trend towards worse relapse-free survival with lower doses
Overall, some cytarabine consolidation is always necessary; in older patients, dose modifications are necessary to prevent excess toxicity
What is the evidence for other maintenance therapy options?
As discussed above, it was clear as early as the 1980s that some kind of consolidation is necessary to prevent a 100% relapse rate
Allogeneic transplant was previously discussed as a sort of “maintenance,” mainly to illustrate graft vs. disease effect - however, maintenance typically refers to lower doses of chemotherapy given over a prolonged period to maintain remission (and ideally cure)
Maintenance was refined in ALL patients and led to higher cure rates in adolescent and later adult populations; unfortunately, when this was tried in AML, none of these approaches worked (aside from high dose cytarabine consolidation)
The older ECOG and German AML studies evaluated cytarabine in combination with other chemotherapies, but failed to show a difference in overall survival
The HOVON group evaluated lenalidomide (an immunomodulatory medication) in a randomized trial but it failed to improve overall survival
A recent NCI trial evaluated nivolumab (a checkpoint inhibitor) in the maintenance setting but also without success
What is the mechanism of action of hypomethylating agents?
Gene expression is regulated through methylation of DNA, which silences gene expression
Many AML cells have mutations in genes that are responsible for controlling gene expression through methylation
These mutations lead to increased methylation in downstream genes responsible for normal cell differentiation and function
These are called “epigenetic” mutations, as the DNA itself is not affected but the mutation leads to excessive methylation
Hypomethylating agents restore gene function by preventing methylation and silencing
Imagine that genes are a series of light switches, which methylation turns off
There are many switches in the off position in AML because of alterations in the epigenetic pathways - but the genes themselves are not mutated!
The hypomethylating agents turn on all the light switches (non-specifically) with the aim of restoring normal gene expression
However, one problem is that certain genes which should be off will be turned on (and vice versa)
The idea is that hypomethylating agents can fix epigenetic issues in AML cells, which have overactive gene silencing via methylation
What is the data behind the use of hypomethylating agents (HMAs) in the maintenance setting for AML?
Researchers knew that hypomethylating agents (e.g. azacitidine and decitabine) were effective in treating AML in older adults and in the refractory setting, so these agents were studied as maintenance options
Several trials evaluated azacitidine maintenance daily x 5 days repeated every 4-6 weeks for one year vs. observation
The first was the AML16 trial from the UK (presented at EHA 2015) which did not demonstrate improvement in overall survival
A 2019 HOVON phase III trial compared azacitidine to observation and showed improved 12 month disease free survival by 10% but still no improvement in overall survival
The ECOG E2906 randomized phase II trial, designed as a pilot study from a parent trial, evaluated decitabine maintenance
The parent study evaluated intermediate dose cytarabine (1.5 g/m2) vs. clofarabine (a purine antimetabolite used in ALL) in consolidation and showed that intermediate dose cytarabine was superior
From the parent study, 120 patients were randomized to decitabine vs. observation for maintenance
There was no statistically significant difference in disease-free survival or overall survival, but there was a trend towards improved DFS
In summary, there was some evidence that disease-free survival might be improved with HMA maintenance, but there was no difference in overall survival
It seems like once the disease does relapse, it tends to be more aggressive
Using HMA in maintenance means it can no longer be used in the relapse setting
What is the QUASAR trial and what are the significant flaws that make it problematic?
This NEJM study included adult patients who underwent intensive chemotherapy and achieved a complete remission (CR) but were not fit for allogeneic stem cell transplant
472 patients were randomized to oral azacitidine or placebo within 4 months of achieving a CR after induction chemotherapy
Double blinded study: neither the investigator and patient knew whether they were on placebo or the trial drug
Patients received maintenance azacitidine on days 1-14 every 28 days
All patients underwent bone marrow biopsies every 3 months for 2 years
If there was evidence of relapse with 5-15% blasts in the marrow, the investigator could add a week of treatment (to days 1-21) in an attempt to deepen the remission
So in the placebo arm, a patient with relapsed AML was having their placebo increased. This seems extremely unethical.
20% of the patients who had relapsed disease had their placebo dose instead of using salvage therapy - this is obviously not standard of care!
Patients were not required to have one or more cycles of high-dose cytarabine (or intermediate dose cytarabine) consolidation
This is a massive limitation of this study. Remember, it was well known by this time that a lack of consolidation or maintenance therapy would result in a 100% relapse rate!
An unacceptable 20% of the patients in the study had no consolidation therapy yet were still able to be randomized to placebo
One last issue is that most of these patients were actually quite fit and should have not had any delay in moving to salvage therapies
65% of all patients received a subsequent therapy and over a third of patients received subsequent intensive chemotherapy at relapse
Despite being a trial of patients “not fit for transplant,” 15% of patients eventually underwent an allogeneic transplant
In the end, there was a statistically significant improvement in both relapse free survival and overall survival with oral azacitidine maintenance compared to placebo
It seems clear that this was driven to a significant degree by a delinquent control arm that fell well short of standard of care
What is the side effect profile of oral azacitidine?
Over 60% of patients had gastrointestinal toxicities with nausea, vomiting, or diarrhea
There was double the rate of severe neutropenia compared to placebo
Nearly half of all patients required dose interruptions due to toxicity
The benefit of maintenance was less impressive in those who got more cycles of consolidation cytarabine
In Figure S2 in the supplementary appendix (page 23), there was no benefit of oral azacitidine in patients who received 3 cycles of consolidation
In the ASH presentation, there was also no benefit for patients who received 2 cycles - this was not shown in the final paper for some reason
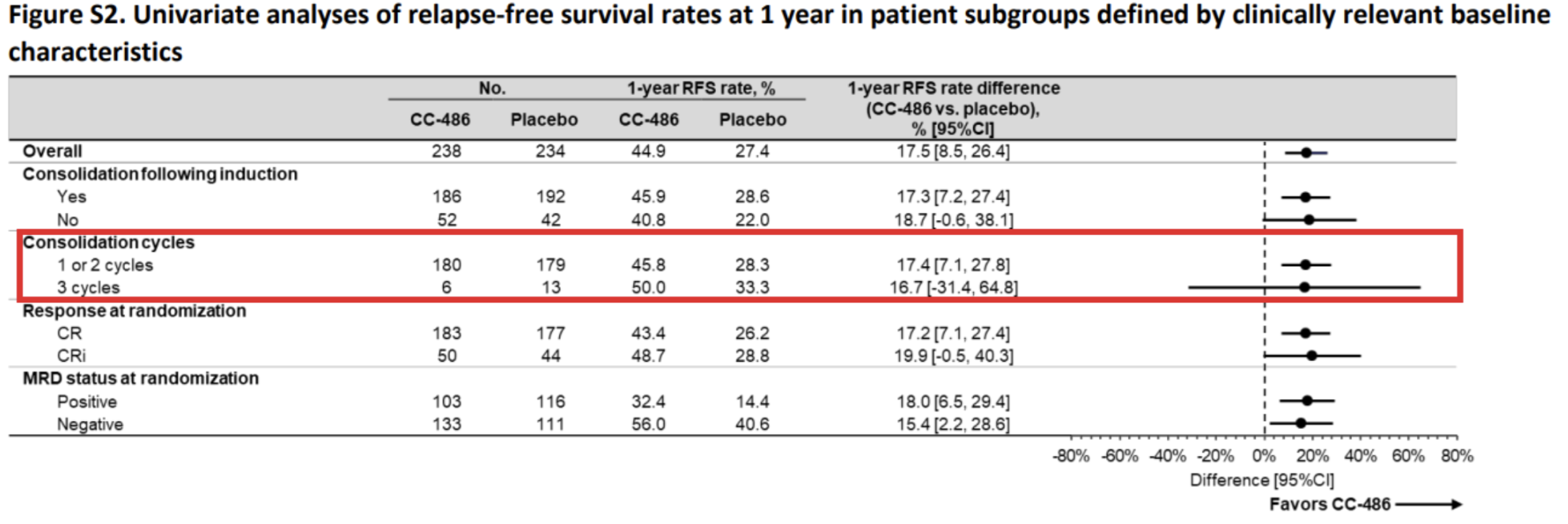
Image Source: Wei, et al., 2020. No copyright infringement intended.
What are the available FLT3 inhibitors?
Historically, the tyrosine kinase inhibitor sorafenib was used to treat FLT3 mutated AML
Sorafenib was the first approved FLT3 targeted agent and has shown utility in the post-transplant maintenance setting
However, it is far less effective than modern drugs such as midostaurin, gilterinib, and quizartinib
Check out our induction episode to review the RATIFY and QuANTUM-First trials which led to the approval of 7+3 + midostaurin and 7+3 + quizartinib
Recall that quizartinib is only used for FLT3 ITD mutations, while midostaurin can be used for FLT3 TKD or ITD mutations
Gilteritinib was FDA approved in the relapsed/refractory setting based on the ADMIRAL trial
This trial will be discussed in more detail later, but showed that gilteritinib is the drug of choice in these patients

What is the data for FLT3 maintenance therapy?
Early data showed the efficacy of sorafenib in the post transplant maintenance setting
The double blind randomized phase II SORMAIN trial published in 2020 randomized 83 patients with FLT3+ AML to sorafenib maintenance vs. placebo after allogeneic transplant
There was a statistically significant improvement in relapse free survival (RFS) and a trend towards improved overall survival
The 24-month RFS was 85% compared to 53% in the placebo arm
Subgroup analysis showed a benefit in MRD positive patients but not MRD negative patients
The most significant limitation of this study is that over 90% of the patients included in the trial did not receive a FLT3 inhibitor in induction
This was not intentional, as the drug was not yet approved, but it does mean that the study is not generalizable to current patients as they would have received midostaurin or quizartinib during induction
Overall, the study showed that if a patient did not receive a FLT3 inhibitor in the induction setting, a FLT3 inhibitor was helpful in the maintenance setting
The results were also likely exaggerated as the study was underpowered, as the original power calculation was for 200 patients
The RADIUS trial evaluated midostaurin in the post-transplant maintenance setting but failed to show improvement in RFS or OS
This perhaps raises the question about why the SORMAIN trial did show benefit
What is the MORPHO trial?
When this trial was accruing, midostaurin was approved in the frontline induction setting and gilteritinib had been approved in the relapsed/refractory setting
Therefore, patients should have received 7+3+midostaurin induction followed by transplant and, in the case of relapse, they should have received salvage gilteritinib
The MORPHO trial published in 2024 randomized 356 patients to gilteritinib vs. placebo for 2 years after transplant
Only 60% of these patients got a FLT3 inhibitor prior to transplant
This was driven by patients enrolled outside of the US, possibly because of lack of approval
There was no statistically significant difference in relapse-free survival or overall survival in the entire population
The 2 year RFS was 77% in the gilteritinib arm vs. 70% in the placebo arm
This 7% difference had a p-value of 0.052 which barely missed the cutoff for statistical significance
Realistically, there probably is some difference, but likely a small one
There was no difference in overall survival (p-value of 0.44) and there was higher non-relapse mortality in the gilteritinib arm
It is also unclear how many patients in the placebo arm received gilteritinib at relapse
This remains an unanswered question: Should FLT3 inhibitors be given in the frontline setting or at relapse?
A post-hoc analysis showed that patients who were MRD positive pre- or post-transplant had a significant RFS benefit with gilteritinib
This was done for prognostic significance - it does not mean that patients who are MRD-positive after induction should not undergo transplant
This episode is sponsored by our Global Research Partners! Click here to get paid to participate in market research surveys!
The crew behind the magic:
Show outline: Vivek Patel
Production and hosts: Ronak Mistry, Vivek Patel, Dan Hausrath
Editing: Resonate Recordings
Shownotes: Neil Biswas
Social media management: Ronak Mistry

We are proud to partner with HemOnc.org!
Want to learn more about the trials that lead to the regimens discussed today? What about dosing schedules? See links in the show notes for a link to HemOnc.org
Have some extra time and want to make some extra money? Click here to get paid to participate in market research surveys!