
Episode 084: Prostate Cancer Series: Pt. 1 - Introduction
Prostate cancer is one of the common cancers diagnosed each year in males. In this new series, we will go through the ins-and-outs of this disease. As medical oncologists, there is so much more to prostate cancer than we see. In our future episodes, we will also highlight the important role of pharmacists, radiation oncologists, and urologists in disease management!
What is the incidence of prostate cancer?
Most common diagnosed cancer in males (27% of all cases in males).
~268,500 new cases in the US.
~ 34,500 or 11% of males with prostate cancer will die but not necessarily from prostate cancer.
Lifetime risk of prostate cancer diagnosis: 12%.
Lifetime risk of prostate cancer death: 3.4%.
~98% of prostate cancer patients survive 5 years.
What are the screening guidelines surrounding prostate cancer?
Key consideration: Prioritize between prostate cancer-related death and all-cause mortality in screening studies.
Dilemma: Assess the necessity of screening for an often-indolent cancer, weighing potential overdiagnosis, unnecessary biopsies, and the stress of a cancer diagnosis against the absence of improved overall survival.
Overlooked aspect: Quality of life not measured in these studies, but crucial, as metastatic prostate cancer significantly impacts it, particularly with the development of painful bone metastases.
Key trials that inform our understanding of screening guidelines:
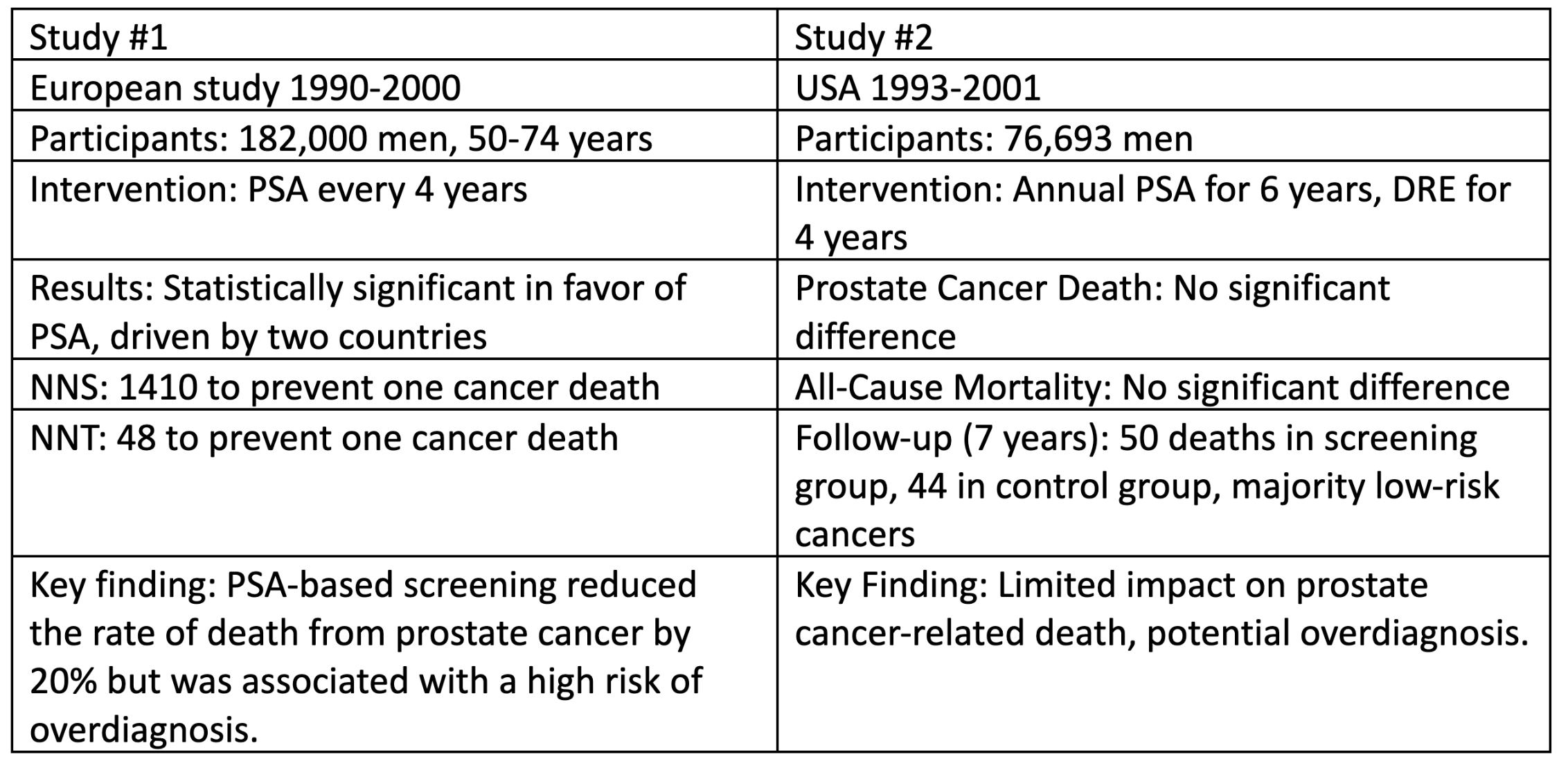
Study 1: https://www.nejm.org/doi/full/10.1056/nejmoa0810084
Study 2: https://www.nejm.org/doi/full/10.1056/NEJMoa0810696
Screen guidelines bottomline:
For average risk patients (no family history or concern for hereditary predispositions): shared decision-making with patients, discuss at around age 50.
Abnormal PSA on routine screening, referred to a urologist for consideration of a biopsy.
Major issues with screening studies:
No improvement in overall survival
Significant difference in prostate cancer death for European study driven by two countries involved which limits generalizability
Most prostate cancer found on imaging is low risk, indolent disease
Overdiagnosis definitely happens
Diagnosis of Prostate Cancer
How is a prostate biopsy performed?
12 cores obtained by urologists, one from each quadrant for minimizing sampling error.
If 50% of cores are positive, this indicates higher risk disease, implying greater infiltration of cancer throughout the prostate.
Many urologists will also recommend Utility of MRI, however universal guidelines about MRIs are not well established

Source: ASCO SEP (No copyright infringement intended)
How is the prostate tissue assessed for disease?
Gleason score:
The quadrants are assessed and assigned a Gleason grade on a scale: 1-5 (1 resembles normal tissue, 5 looks very abnormal).
Typically reported grades: 3-5; 1-2 considered essentially normal tissue.
The two most prevalent grades are reported in an “X+Y” manner and are called the Gleason score:
First, the most predominant grade on malignant cores.
Second, the second most common grade on malignant cores.
Single grade pattern: both numbers are same.
Higher combined score signifies more aggressive disease.
The International Society of Urological Pathology (2014) created a revised system called Group Grades to simplify things:

Source: https://www.pcf.org/about-prostate-cancer/diagnosis-staging-prostate-cancer/gleason-score-isup-grade/ (No copyright infringement intended).
How do we risk stratify patients?
The critical components needed:
Number of cores (at least 12 sampled)
Combined Gleason score
Percentage of the cores involved by cancer
TFOC Tips to stratify patients:

*Think of Andrew Jackson on the $20 bill. Picture Andrew Jackson having a bad prostate in your head. PSA > 20 is high risk!
What are other features on our biopsy report to pay attention to?
>95% of cases are going to be adenocarcinoma!
Intraductal/cribriform → higher risk
Seminal vesicle/capsule invasion → higher risk (Changes T staging!)
Fragmented cores → If cores are fragmented, there is the potential to overestimate the amount of disease.
What are key characteristics on physical exam?
Clinical exam on DRE:
NO palpable mass: T1
Palpable mass: T2
How do we stage prostate cancer using the TNM staging?
Link to TNM staging guidelines can be found here
Unique aspects of TNM staging in prostate cancer to pay attention to:
Incorporation of pathologic details: Utilizes pathologic information, including grade and patient's PSA.
N1 disease: Stage IVA.
Any other distant disease, whether nodal or involving other structures: Stage IVB.
Great graphics to reference when trying to assess extent of nodal disease: https://radiologyassistant.nl/abdomen/prostate/prostate-cancer-pi-rads-v2-1-1
Arguably more important than the TNM staging in localized disease is how we decide what additional testing is needed. The NCCN guidelines lay this out nicely:

Source: NCCN prostate cancer guidelines
Key takeaways from this chart: For unfavorable intermediate and higher —> Obtain bone and soft tissue imaging/PSMA PET scans!
What are the highlights of how we treat patients with prostate cancer?
Observation: minimal symptoms, life expectancy <10y. If symptoms arise in the future, consider palliative approach given limited life expectancy.
Active surveillance: in those with life expectancy >10 years: biopsies as needed, PSA monitoring, imaging. Unlike observation, active surveillance may warrant treatment in future.
Radical prostatectomy with pelvic lymph node dissection. Employed in unfavorable intermediate risk groups and higher.
External Beam Radiation Therapy (discussions with Radiation Oncology colleagues in subsequent episodes)
Brachytherapy (seeds implanted in prostate cancer bed)
Androgen Deprivation Therapy (to decrease testosterone levels).
What else happens after surgery or radiation therapy for localized prostate cancer?
Goal after surgery is an undetectable PSA
Administer ADT if: Lymph node involvement at the time of surgery (often done/managed by urology)
Administer ADT + abiraterone If: Very high risk features:
Extra prostatic extension to the seminal vesicles or further.
Gleason >9
PSA rise after surgery: Rule out distance mets and refer for radiation therapy.
If PSA >2 points after radiation: Relapsed disease.
What are some key terms in the management of prostate cancer?
Castration sensitive = testosterone > 50
Includes patients with no ADT exposure or inadequate ADT exposure
Castration resistant = testosterone < 50
Patients who have progressed despite adequate ADT
M0 biochemical recurrence = PSA rising without evidence of metastatic disease on imaging
If any PSA rise after surgery, we proceed with salvage radiation after ruling out metastatic disease
Post radiation: PSA rise greater than 2 ng/mL above the nadir
Some of these patients with PSA rise after radiation and no metastatic disease on imaging (M0 biochemical recurrence) still have an indolent course and we assess the rate of increase in PSA to determine next treatment steps
M1 disease = PSA rising and imaging shows metastatic disease
Combining castration status with either M0 or M1 disease will dictate our therapy
Castration sensitive M0 biochemical recurrence
Castration resistant M0 biochemical recurrence
Castration sensitive M1 prostate cancer (i.e. metastatic prostate cancer)
Castratation resistant M1 prostate cancer
References:
NCCN Guidelines: Prostate Cancer
The crew behind the magic:
Show outline: Ronak Mistry, Vivek Patel
Production and hosts: Ronak Mistry, Vivek Patel, Dan Hausrath
Editing: Resonate Recordings
Shownotes: Srijan Valasapalli
Social media management: Ronak Mistry