
Episode 129: Testicular Cancer Series, Pt 3 - Disseminated and relapsed/refractory disease
This week, we talk all about disseminated testicular cancer, highlighting our current treatment modalities and why we do what we do. We also cover refractory disease. This episode builds on our prior discussions in Parts 1 and 2, so be sure to check these out if you haven’t already!
A review of risk stratification
As discussed previously in Part 1, we need to divide patients into favorable risk, intermediate risk, and poor risk
Remember the first step is to determine seminoma vs non seminoma
Then divide into stage 1, 2 or 3 based on sites of disease
Then use the location of tumor and post orchiectomy tumor marker nadir to stratify
Where did his stratification come from?
Stratification system was developed by the International Germ Cell Cancer Collaborative Group (IGCCCG) and published in 1997 [1]
One of the most important retrospective studies in testicular cancer
Examined survival outcomes of > 5000 patients with metastatic germ cell tumors treated from 1975 – 2000 with purpose to identify statistically significant prognostic clinical factors
Adverse factors for non-seminoma:
Mediastinal primary site
Presence of non-pulmonary visceral metastases (such as liver, bone and brain)
Degree of elevation of AFP, β-hCG, and LDH
Adverse factors for seminoma:
Presence of non-pulmonary visceral metastases (such as liver, bone and brain)
Integration of those factors for prognosis:
Good prognosis (60% patients): 91% 5-year survival rate
Intermediate prognosis (26%): 79% 5-year survival rate
Poor prognosis (14%): 48% 5-year survival rate
This practical model was validated using the British Medical Research Council (MRC), the European Organization for Research and Treatment of Cancer (EORTC), and Eastern Cooperative Oncology Group/Southwest Oncology Group/Cancer and Leukemia Group B Trial in GCT (ECOG/SWOG/CALGB) databases


Image sources: Figures 1 and 2. Image source: IGCCCG 1997. No copyright infringement intended
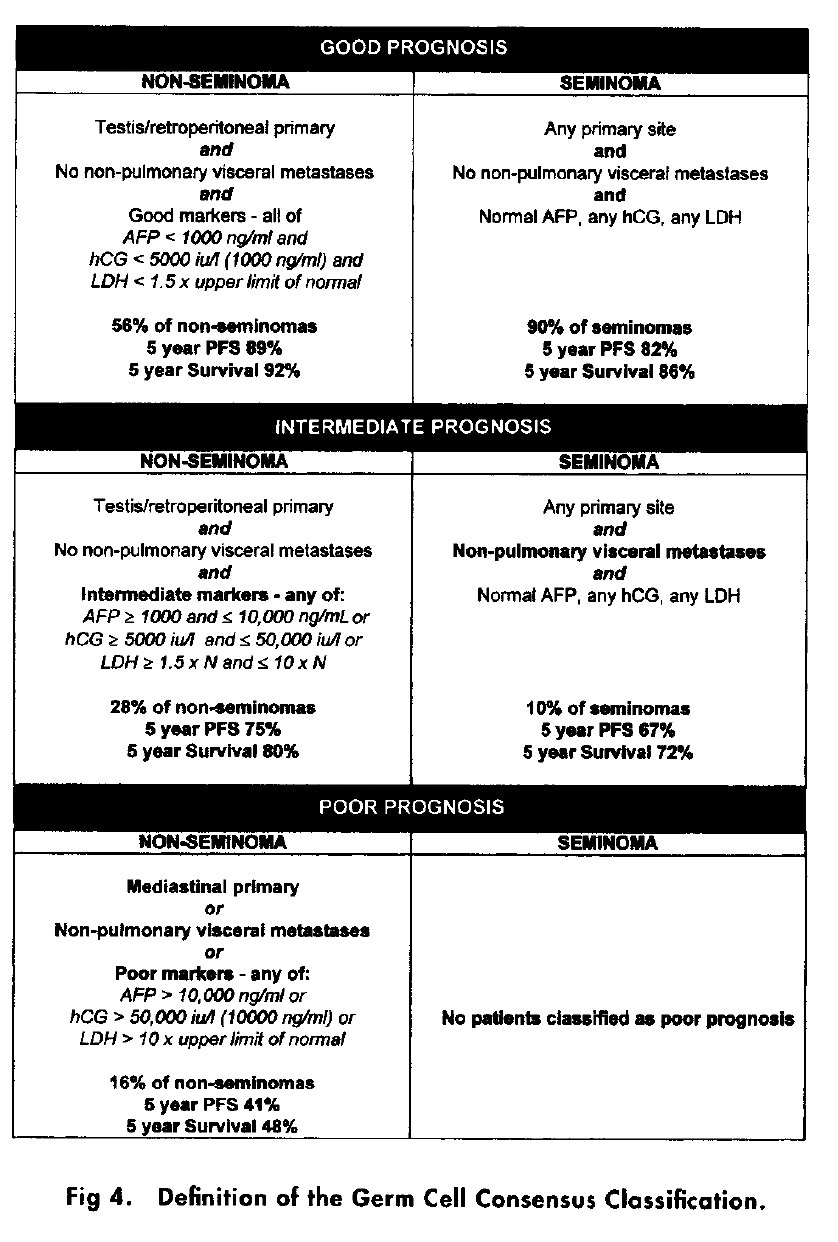
Image source: Figure 4. Risk stratification from IGCCCG 1997. No copyright infringement intended
Updated prognostic system published in 2021 that provided a more accurate estimation of survival compared to original IGCCCG [2]
Examined survival outcomes of > 9000 patients with metastatic nonseminomatous germ cell tumors treated from 1990 – 2013
Primary endpoints were progression-free survival (PFS) and overall survival (OS)
A more granular prognostic model was developed with additional adverse factors:
New cutoff of LDH as 2.5x upper limit of normal (ULN)
Increasing age
Presence of lung metastases
Good prognosis (original vs updated):
5- year PFS similar 89% vs 90%
5-year OS increased from 92% to 96%
Intermediate prognosis (original vs updated):
5- year PFS similar 75% vs 78%
5-year OS increased from 80% to 89%
Poor prognosis (original vs updated):
5- year PFS increased from 41% to 54%
5-year OS increased from 48% to 67%
Click for access to online risk stratification calculator
For Seminoma:
Only good risk and intermediate risk as we generally don’t have tumor marker elevation
Good Risk: Isolated disease, retroperitoneal LN involvement, and/or lung involvement
Intermediate Risk: any metastatic disease outside of the retroperitoneal LN or the lungs
Remember that pelvic LN involvement with an inguinal LN would be higher risk given that these germ cell tumors should follow the anatomic lymph drainage system and go to retroperitoneal LN
Non-Seminoma:
Use the nadir value of tumor markers AFP, β-hCG, and LDH as well as location to risk stratify
Good risk: AFP < 1000, β-hCG < 5000, or LDH < 1.5x ULN
Intermediate Risk: AFP > 1000, β-hCG > 5000, or LDH > 1.5x ULN
Poor Risk: AFP > 10K, β-hCG > 50K, or LDH > 10x ULN; primary mediastinal germ cell tumor, non-pulmonary visceral metastases
Can use mnemonic 1, 5, 1.5 as intermediate and poor risk are treated the same so remember AFP > 1000, β-hCG > 5000, or LDH > 1.5x ULN
How did we get to BEP x 4 cycles regimen?
Indiana University developed a regimen in 1974 consisting of Cisplatin + Vinblastine + bleomycin (PVB) x 12 weeks followed by vinblastine maintenance to complete 2 years. [3]
60% cure rate which was significantly higher than historical standard of 5%
However, lots of toxicities related to vinblastine: myalgias, constipation, paralytic ileus, severe granulocytopenia and potential sepsis
Subsequent PVB study tested the utilization of maintenance therapy to prevent relapse. [4]
Standard arm of 21 months of maintenance vinblastine (total 2 years chemotherapy) vs 12 weeks of PVB with no further therapy
There was a 9% relapse rate during maintenance with vinblastine and a 7% relapse rate with no maintenance therapy
The overall relapse rate was 8%.
Indicates that maintenance therapy is unnecessary in disseminated testicular cancer.
For patients who relapsed, the salvage regimen of cisplatin + VP-16 (i.e. etoposide) was introduced in 1978.[5]
33 patients with advanced refractory germinal neoplasms treated with VP-16 alone or in combination with cisplatin, bleomycin and frequently adriamycin
There were 14 complete and 15 partial remissions
So the thought was to include Etoposide + Cisplatin in upfront treatment
Randomized study from 1981-1984 comparing PVB vs cisplatin + VP-16 + bleomycin (PVP16B now known as BEP)[6]
Therapeutic results were similar with no evidence of disease (NED) 74% with PVD and 83% with PVP16B.
However, highly statistically significant reduction in myalgias and peripheral neuropathy with PVP16B
This led to BEP given every 21 days for 4 cycles (I.e. 12 weeks) becoming the standard of care
How often are each of these drugs actually given during this regimen?
Bleomycin is given weekly
Etoposide and cisplatin are given daily on Day 1-5 and repeated every 21 days
Logistically challenging:
Lots of infusion visits for a young patient but results in very high cure rates
Patients with intermediate to poor risk will be given this regimen for 4 cycles
What is the VIP x 4 cycle regimen (VIP = Vinblastine + Ifosfamide + Cisplatin)?
Ifosfamide had been shown to have excellent single agent activity and could produce cure in the salvage setting when combined in roughly 25-35% of patients.[7-8]
This led to a randomized study of BEP x 4 cycles vs VIP x 4 cycles published in 1998. [9]
The study enrolled over 300 patients with poor risk disseminated germ cell tumor
Overall complete remission rate (VIP 37 %, BEP 31%). Not statistically different
Favorable response rate (VIP 63%, BEP 60%). Not statistically different
Failure free at 2 years (VIP 64%, BEP 60%). Not statistically different
2-year overall survival (VIP 74%, BEP 60%). Not statistically different
VIP had significantly more toxicity with more grade 3 or higher hematologic toxicity and GU toxicity despite the use of mesna
There was another randomized study run by the EORTC concurrently comparing BEP vs VIP [10]
Over 80 patients with intermediate prognosis
Complete response (CR) rate (VIP 74%, BEP 79%). Not statistically different
5-year PFS (VIP 85%, BEP 83%. Not statistically different
VIP had significantly more hematologic toxicity
Study terminated early after results of poor risk trial came out
These studies demonstrated that efficacy outcomes are similar but the pulmonary toxicity of BEP does not outweigh the other toxicities of VIP
CAVEAT: VIP is favored over BEP for primary mediastinal germ cell tumors
This is based on a study published out of Indiana University in 2021.[11]
Looked at outcomes for patients with primary mediastinal germ cell tumor
There were 255 patients included in the study with primary mediastinal nonseminomatous germ cell tumor
The important thing to remember is that all non-seminoma patients with residual tumor after chemotherapy must undergo resection given possibility of a component of teratoma which is chemotherapy resistant
Did the use of bleomycin impact surgical outcomes?
Post-operative ARDS occurred in 11% of patients and 4% of patients died from ARDS
The incidence of ARDS with BEP was about 15% compared to only 2.5% with VIP
This data really shows that we should be recommending VIP x 4 cycles for primary mediastinal germ cell tumors given that most patients require resection and the rate of postoperative ARDS is high with BEP leading to increased morbidity and mortality
Fellow on Call Takeaways:
For patients with intermediate or poor risk disseminated germ cell tumor, we give BEP x 4 cycles which is 12 weeks of therapy
After chemotherapy, resection of all residual tumors for non-seminoma is mandatory
For primary mediastinal germ cell tumor, by definition is poor risk, we often prefer VIP x 4 cycles given risk of postoperative ARDS with BEP x 4 cycles
How did we get to BEP x 3 cycles or EP x 4 cycles for favorable risk patients?
Push to de-escalate therapy in the young patient population given risk for long-term neuropathy and ototoxicity with cisplatin and potential treatment related MDS and AML with etoposide
This led to a randomized trial in favorable risk patients comparing BEP x 4 cycles vs BEP x 3 cycles published in JCO in 1989.[12]
184 patients entered the trial and all had a minimal follow up of 1 year
Disease free status (3 cycles 98% vs 4 cycles 97%). Not statistically different
The deletion of the 4th cycle significantly reduced toxicity, cost and inconvenience of the curative regimen
Led to BEP x 3 cycles becoming the standard of care for favorable risk patients
The regimen Etoposide + Cisplatin (EP) x 4 cycles has never been compared to BEP x x3 cycles in a randomized trial
The regimen EP x 4 cycles comes from a randomized study comparing Etoposide + Cisplatin x 4 cycles to Etoposide + carboplatin x 4 cycles published in JCO in 1993.[13]
270 favorable risk patients were enrolled
CR achieved in 88% of patients receiving Etoposide + Carboplatin (EC) vs 90% receiving EP
Relapse from CR occurred in 12% EC vs 3 % EP
Therefore 24% EC experienced incomplete response or relapse compared to 13% EP
EC was inferior to therapy with EP
EP numerically has similar outcomes to BEP x 3 cycles
A retrospective study from Indiana University looked at differences in outcomes for EP x 4 cycles compared to BEP x x3 cycles that was published in 2018. [14]
The study is difficult to interpret given that it was retrospective and patient selection likely played a role
Ultimately there was no statistically significant difference in 10-year overall survival
EP x 4 cycles (91%) vs BEP x 3 cycles (98%)
Long term survival was over 90% in both groups
Fellow on Call Takeaways:
For favorable risk, we have BEP x 3 cycles (9 weeks of therapy) or EP x 4 cycles (12 weeks of therapy) and both regimens are reasonable given lack of prospective randomized data
This also means we can drop the bleomycin for pulmonary toxicity and finish out a regimen with EP x 4 cycles
For intermediate or poor risk, we have BEP x 4 cycles or VIP x 4 cycles.
If there is pulmonary toxicity you would switch to VIP to complete treatment course
Do we need to resect residual masses in pure seminoma?
For patients with residual disease < 3 cm: Observation is very with serial imaging as most are just tumor necrosis and here we are not worried about teratoma
For patients with residual disease > 3 cm: obtain a PET/CT (which has a 94% negative predictive value) and proceed with biopsy or resection if PET avid
Fellow on Call Takeaways:
Non-seminoma requires resection for residual masses but seminoma does not
If there is significant tumor growth during chemotherapy then you should proceed to resection for growing teratoma syndrome as opposed to continuing chemotherapy
How to approach relapsed and/or refractory disease
The timing of relapse and amount of relapsed disease matters:
If relapse is localized and occurs > 2 years after initial treatment, then surgical resection is preferred
If relapse is within 2 years of initial treatment or disseminated disease, then salvage chemotherapy is preferred
Chemotherapy treatment options:
There are 2 pivotal phase II trials evaluation Taxol + Ifosfamide + cisplatin (TIP) x 4 cycles and Vinblastine + Ifosfamide + Cisplatin (VeIP) x 4 cycles as salvage therapy
TIP Regimen [15]
46 patients treated with TIP after prior CR to first line chemotherapy. All patients with testis primary tumor site and favorable prognostic factors
63% durable CR rate and a 2-year PFS of 65%
VeIP Regimen [16]
132 patients with progressive, disseminated germ cell tumors after Cisplatin – Etoposide based induction therapy
Overall durable CR rate of 24%
However, for relapsed primary mediastinal non seminomatous germ cell tumors the durable CR rate was 0%
Both VeIP and TIP x 4 cycle are reasonable options for salvage therapy with TIP showing numerically better results albeit in a more favorably selected patient population
What treatment options do we have in the 3rd line setting?
Option 1: Single center study from Indiana University published in NEJM in 2007 [17]
184 patients with either relapsed or refractory germ cell tumors:
75% of the patients were in the 2nd line setting
20% were platinum refractory
Treated with high dose Carboplatin (700 mg/m2) + Etoposide (750 mg/m2) followed by stem cell rescue
After recovery, they did it again so the patient gets a tandem autotransplant rescue
Overall durable CR rate was 63% (similar to the TIP data) but in a much higher risk population with a significant proportion of platinum refractory disease
Durable CR rate of 70% in patients who received the treatment as 2nd line therapy
Durable CR rate of 45% in patients who received the treatment as 3rd line therapy or later
Durable CR rate of 68% in patients who were platinum sensitive
Durable CR rate of 45% in patients who were refractory to standard dose platinum
Option 2: Single center study from Memorial Sloan Kettering using a different regimen published in JCO in 2007 [18]
48 patients entered who had progressive germ cell tumor and unfavorable prognostic features after chemotherapy
Patients received Paclitaxel + Ifosfamide x 2 cycles + stem cell collection then Carboplatin + Etoposide x 3 cycles with autologous stem cell rescue
Patients got a triplet auto transplant essentially
Durable CR of 51%
On the horizon: TIGER is an International phase III trial to establish the standard of care for second-line chemotherapy in patients with advanced germ cell tumors
Compares initial salvage conventional-dose chemotherapy with the TIP regimen vs. high-dose chemotherapy and autologous stem cell transplant with the TI-CE regimen (using MSK approach) with a primary endpoint of overall survival.
Ongoing trial but should have publishable data in the next year or so
References:
1. International Germ Cell Consensus Classification: a prognostic factor-based staging system for metastatic germ cell cancers. International Germ Cell Cancer Collaborative Group. J Clin Oncol. 1997;15(2):594-603. https://ascopubs.org/doi/abs/10.1200/JCO.1997.15.2.594
2. Gillessen S, Sauvé N, Collette L, et al. Predicting Outcomes in Men With Metastatic Nonseminomatous Germ Cell Tumors (NSGCT): Results From the IGCCCG Update Consortium [published correction appears in J Clin Oncol. 2022 Jul 10;40(20):2283. doi: 10.1200/JCO.22.01243.]. J Clin Oncol. 2021;39(14):1563-1574.https://ascopubs.org/doi/full/10.1200/JCO.20.03296?af=R
3. Einhorn LH, Donohue J. Cis-diamminedichloroplatinum, vinblastine, and bleomycin combination chemotherapy in disseminated testicular cancer. Ann Intern Med. 1977;87(3):293-298. https://www.acpjournals.org/doi/10.7326/0003-4819-87-3-293?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed
4. Einhorn L H, Williams S D, Troner M, Greco F A, Birch R. N Engl J Med. 1981;305:717–731. https://www.nejm.org/doi/10.1056/NEJM198109243051303?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed
5. Williams SD, Einhorn LH, Greco FA, Oldham R, Fletcher R. VP-16-213 salvage therapy for refractory germinal neoplasms. Cancer. 1980;46(10):2154-2158. https://acsjournals.onlinelibrary.wiley.com/doi/epdf/10.1002/1097-0142%2819801115%2946%3A10%3C2154%3A%3AAID-CNCR2820461008%3E3.0.CO%3B2-3
6. Williams SD, Birch R, Einhorn LH, Irwin L, Greco FA, Loehrer PJ. Treatment of disseminated germ-cell tumors with cisplatin, bleomycin, and either vinblastine or etoposide. N Engl J Med. 1987;316(23):1435-1440. https://www.nejm.org/doi/pdf/10.1056/NEJM198706043162302
7. Wheeler BM, Loehrer PJ, Williams SD, Einhorn LH. Ifosfamide in refractory male germ cell tumors. J Clin Oncol. 1986;4(1):28-34. https://ascopubs.org/doi/10.1200/JCO.1986.4.1.28?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed
8. Loehrer PJ Sr, Einhorn LH, Williams SD. VP-16 plus ifosfamide plus cisplatin as salvage therapy in refractory germ cell cancer. J Clin Oncol. 1986;4(4):528-536. https://ascopubs.org/doi/10.1200/JCO.1986.4.4.528?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed
9. Nichols CR, Catalano PJ, Crawford ED, Vogelzang NJ, Einhorn LH, Loehrer PJ. Randomized comparison of cisplatin and etoposide and either bleomycin or ifosfamide in treatment of advanced disseminated germ cell tumors: an Eastern Cooperative Oncology Group, Southwest Oncology Group, and Cancer and Leukemia Group B Study. J Clin Oncol. 1998;16(4):1287-1293.https://ascopubs.org/doi/10.1200/JCO.1998.16.4.1287?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed
10. de Wit R, Stoter G, Sleijfer DT, et al. Four cycles of BEP vs four cycles of VIP in patients with intermediate-prognosis metastatic testicular non-seminoma: a randomized study of the EORTC Genitourinary Tract Cancer Cooperative Group. European Organization for Research and Treatment of Cancer. Br J Cancer. 1998;78(6):828-832. https://pmc.ncbi.nlm.nih.gov/articles/PMC2062963/pdf/brjcancer00006-0134.pdf
11. Kesler KA, Stram AR, Timsina LR, Turrentine MW, Brown JW, Einhorn LH. Outcomes following surgery for primary mediastinal nonseminomatous germ cell tumors in the cisplatin era. J Thorac Cardiovasc Surg. 2021;161(6):1947-1959.e1. https://www.sciencedirect.com/science/article/pii/S0022522320309958
12. Einhorn LH, Williams SD, Loehrer PJ, et al. Evaluation of optimal duration of chemotherapy in favorable-prognosis disseminated germ cell tumors: a Southeastern Cancer Study Group protocol. J Clin Oncol. 1989;7(3):387-391. https://ascopubs.org/doi/10.1200/JCO.1989.7.3.387
13. Bajorin DF, Sarosdy MF, Pfister DG, et al. Randomized trial of etoposide and cisplatin versus etoposide and carboplatin in patients with good-risk germ cell tumors: a multiinstitutional study. J Clin Oncol. 1993;11(4):598-606. https://ascopubs.org/doi/10.1200/JCO.1993.11.4.598
14. Cary C, Jacob JM, Albany C, et al. Long-Term Survival of Good-Risk Germ Cell Tumor Patients After Postchemotherapy Retroperitoneal Lymph Node Dissection: A Comparison of BEP × 3 vs. EP × 4 and Treating Institution. Clin Genitourin Cancer. 2018;16(2):e307-e313. https://www.sciencedirect.com/science/article/abs/pii/S1558767317303142#:~:text=The%2010%2Dyear%20OS%20for,10
15. Kondagunta GV, Bacik J, Donadio A, et al. Combination of paclitaxel, ifosfamide, and cisplatin is an effective second-line therapy for patients with relapsed testicular germ cell tumors. J Clin Oncol. 2005;23(27):6549-6555. https://ascopubs.org/doi/10.1200/JCO.2005.19.638
16. Loehrer PJ Sr, Gonin R, Nichols CR, Weathers T, Einhorn LH. Vinblastine plus ifosfamide plus cisplatin as initial salvage therapy in recurrent germ cell tumor. J Clin Oncol. 1998;16(7):2500-2504. https://ascopubs.org/doi/10.1200/JCO.1998.16.7.2500
17. Einhorn LH, Williams SD, Chamness A, Brames MJ, Perkins SM, Abonour R. High-dose chemotherapy and stem-cell rescue for metastatic germ-cell tumors. N Engl J Med. 2007;357(4):340-348. https://www.nejm.org/doi/full/10.1056/NEJMoa06774
18. Kondagunta GV, Bacik J, Sheinfeld J, et al. Paclitaxel plus Ifosfamide followed by high-dose carboplatin plus etoposide in previously treated germ cell tumors [published correction appears in J Clin Oncol. 2007 May 20;25(15):2149]. J Clin Oncol. 2007;25(1):85-90. https://ascopubs.org/doi/10.1200/JCO.2006.06.9401?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed
The crew behind the magic:
Show outline: Vivek Patel
Production and hosts: Ronak Mistry, Vivek Patel, Dan Hausrath
Editing: Resonate Recordings
Shownotes: Matt Barke, Agrima Mian
Social media management: Ronak Mistry

We are proud to partner with HemOnc.org!
Want to learn more about the trials that lead to the regimens discussed today? What about dosing schedules? See links in the show notes for a link to HemOnc.org
Have some extra time and want to make some extra money? Click here to get paid to participate in market research surveys!