
Episode 133: VTE Series - Perioperative Anticoagulation Management and Emergent Reversal
This week, we discuss another set of high yield topic for anyone who cares for patients on anticoagulation - how to safely hold anticoagulation prior to a procedure and how to reverse the effects of the drug in the even of an emergent situation. We discuss our approach to how we discuss this with our patients and our medical colleagues! Dan also shares his dotphrases for your reference!
How do we manage patients’ anticoagulation ahead of an invasive procedure (e.g. biliary stent exchange)?
Always ask about planned procedures at yearly check-in appointments
If possible, always ask for a 4-6 week notice to allow adequate time to plan
Only the team performing the procedure will know the bleeding risk of a specific procedure, and whether or not anticoagulation needs to be held
You will be able to guide on how urgently the patient needs to restart anticoagulation based on the risk of the VTE
In general, procedure teams will want about:
5 days for warfarin or fondaparinux washout
1 day for low risk bleeding procedures for DOAC; 2 days for higher risk bleeding procedures for DOAC (all assuming normal renal function) (PAUSE Study)
24 hours for enoxaparin washout (last dose the AM prior to procedure)
30 minutes - 4 hours for heparin washout (depending on the procedure’s bleeding risk and the proceduralist’s preference)
Argatrobran is similar to heparin with a slightly shorter half-life => 1-2 hours of washout is generally sufficient
1-2 hours for bivalirudin (clearance time depends on renal function, half-life is 30-60 mins)
In all cases, we always recommend discussions with the proceduralist service to confirm their preference and to have a conversation about the risks and benefits of holding anticoagulation for your patient.
What about “bridging anticoagulation”? How do we select patients for bridging?
Some patients will need as little interruption in anticoagulation as possible and can be “bridged” off their longer-acting anticoagulant with enoxaparin or even heparin
Patients who DO NOT require bridging anticoagulation:
For most patients, there is no need to bridge if the primary indication for anticoagulation is:
Atrial fibrillation / atrial flutter (AF)
VTE with most recent event >3 mo ago
This is based on the BRIDGE and PERIOP-2 trials from cardiology literature
BRIDGE:
Enrolled 1900 patients on warfarin for AF
Excluded patients with recent embolism, recent TIA, and mechanical valves
Patients randomized to bridge with dalteparin vs placebo
There was no difference in embolic event in 30 days after procedure (0.3 vs 0.4%) and a significant increase in major bleeding with bridging (3.2 vs 1.3%)
Significant increase in 2ndary outcome of major bleeding (3.2 vs 1.3%)
PERIOP-2
Enrolled ~1500 patient on warfarin for AF
Included patients with mechanical valves (21% of enrolled patients)
Patients were bridged off anticoagulation before surgery with dalteparin and then randomized to dalteparin bridge (to a target INR >2) vs. placebo after surgery
There was no difference in thromboembolism for either AF (1.41% vs 0.75%) or MV (0% vs 0.67%) groups
There was no difference for major bleeding (AF: 2.62 vs 1.64%, MV: 1.96% vs 0.67%)
Patients who require bridging anticoagulation:
VTE with recent event (<3 months ago)
Consider delaying procedure until >3 months from the VTE date if possible (or at least >4-6 weeks from VTE date)
Recurrent VTE with prior thrombosis during short-duration of anticoagulation interruption
Patients at high risk for VTE
Antithrombin III deficiency
Triple positive APS
Select cases with thromboses secondary to estrogen-containing OCPs
Personal history of warfarin skin necrosis
Specific cardiac indications (usually in consultation with cardiology)
Mechanical mitral/aortic valves
Recent AF-associated embolic stroke (excluded from trials looking at safety of holding anticoagulation without bridge)
Recent PCI on single antiplatelet therapy + anticoagulation
How do we bridge patients’ anticoagulation?
For most patients, we use enoxaparin for bridging, which can start after the second or third missed dose of anticoagulant
For warfarin, we recommend they take the first enoxaparin at the time due for their second missed dose
For DOAC (in the select cases where patients are very high risk for thrombosis off of anticoagulation), we recommend they take the first enoxaparin at the time due for their third missed dose
Make sure to outline your bridging plan in explicit detail (see sample Smartphase below)

Courtesy of Dan Hausrath
Challenging Scenarios with Bridging Anticoagulation
Some patients will have a contraindication for enoxaparin due to a history of HIT or poor renal function
For these patients, we recommend either hospital admission for bridging with heparin (poor renal function) or bridging with bivalirudin (history of HIT)
Some patients will have an exceedingly high risk of recurrent VTE off anticoagulation
For these patients, we generally will provide standard enoxaparain bridge followed by admission for 24-hour heparin infusion prior to the procedure to minimize the time window off anticoagulation
Reversing Anticoagulation (in the case of major bleeding)
DOACs
After resuscitation with blood products and fluids, we recommend obtaining an anti-Xa level to determine whether or not anticoagulant is present in the bloodstream (or a modified thrombin time assay for patients on dabigatran)
If the level comes back undetectable, there is no role for attempts at reversal
If the level is detectable (suggesting anticoagulant in circulation), then we can attempt reversal:
For dabigatran, there is a reversal agent called idarucizumab or “Praxbind” (monoclonal antibody specific to dabigatran), but this may not be available at some centers
For the Xa inhibitors, there is an approved reversal agent andexanet alfa or “Andexxa” that works as a dummy protein of factor Xa (competitively inhibits DOAC effects), but this is not readily available at most tertiary care centers
In practice, for patients with life-threatening bleeds, we tend to give prothrombin complex concentrate to overwhelm the effect of the DOAC with excess clotting factors
Ciraparantag has shown promise as a potentially more viable reversal agent, but is still under investigation in early phase trials
Warfarin
Warfarin (as a vitamin K antagonist depleting factors II, VII, IX, and X along with protein C and S) can be reversed by replacing the missing factors and providing vitamin K to resume normal production of these factors
Obtain an INR level upfront to guide reversal
PCC contains the clotting factors depleted by warfarin and can be administered for reversal without the volume required with FFP to achieve the same degree of reversal
PCC may contain heparin -> for patients with a history of HIT, vitamin K and FFP can be administered in combination instead
Heparins
Heparins can be reversed with protamine, but this can be tricky and is less effective for LMWH compared to UFH (see guidance on protamine reversal strategy below)
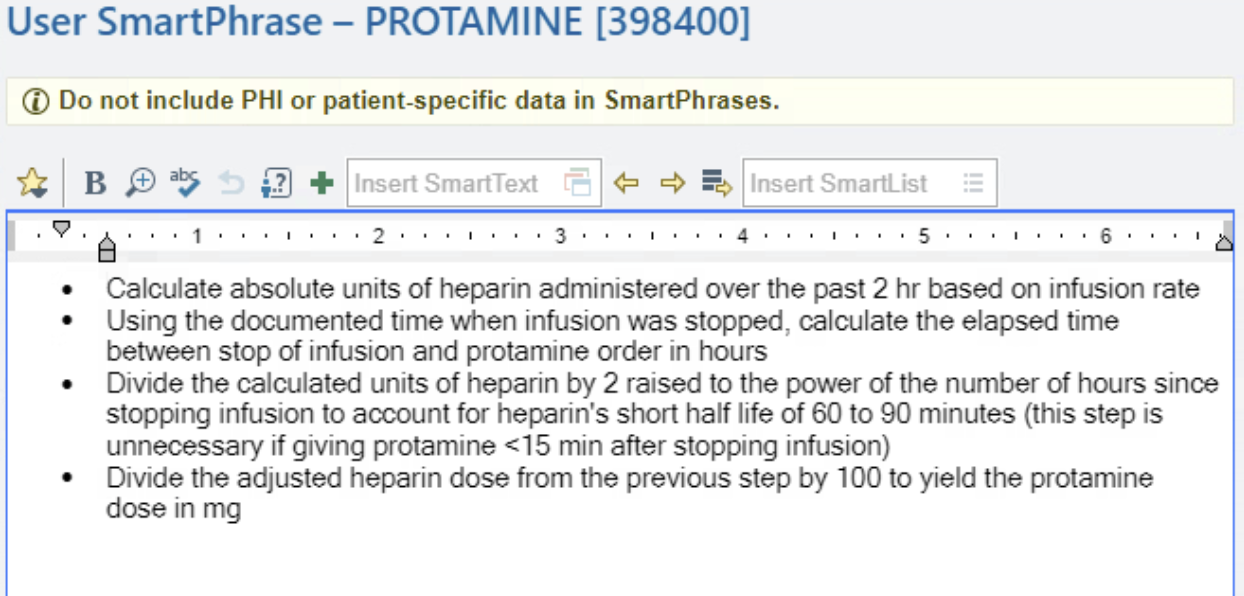
Courtesy of Dan Hausrath
Fondaparinux
Fondaparinux behaves more like a DOAC and is not adequately reversed with protamine (use the DOAC reversal strategies discussed above)
References:
BRIDGE: Douketis, J. D., Spyropoulos, A. C., Kaatz, S., Becker, R. C., Caprini, J. A., Dunn, A. S., Garcia, D. A., Jacobson, A., Jaffer, A. K., Kong, D. F., Schulman, S., Turpie, A. G. G., Hasselblad, V., & Ortel, T. L. (2015). Perioperative bridging anticoagulation in patients with atrial fibrillation. New England Journal of Medicine, 373(9), 823–833. https://doi.org/10.1056/nejmoa1501035
PERIOP-2: Kovacs, M. J., Wells, P. S., Anderson, D. R., Lazo-Langner, A., Kearon, C., Bates, S. M., Blostein, M., Kahn, S. R., Schulman, S., Sabri, E., Solymoss, S., Ramsay, T., Yeo, E., & Rodger, M. A. (2021). Postoperative low molecular weight heparin bridging treatment for patients at high risk of arterial thromboembolism (PERIOP2): Double blind randomised controlled trial. BMJ. https://doi.org/10.1136/bmj.n1205
PAUSE: Douketis, JD, et. al. (2019). Perioperative Management of Patients With Atrial Fibrillation Receiving a Direct Oral Anticoagulant. JAMA Internal Medicine. 179(11):1469-1478. doi:10.1001/jamainternmed.2019.2431
The crew behind the magic:
Show outline: Daniel Hausrath
Production and hosts: Ronak Mistry, Vivek Patel, Dan Hausrath
Editing: Resonate Recordings
Shownotes: Karam Elsolh
Social media management: Ronak Mistry

We are proud to partner with HemOnc.org!
Want to learn more about the trials that lead to the regimens discussed today? What about dosing schedules? See links in the show notes for a link to HemOnc.org
Have some extra time and want to make some extra money? Click here to get paid to participate in market research surveys!