
Episode 073: Management of Early Stage Diffuse Large B-Cell Lymphoma (DLBCL)
This week, we continue our conversation about DLBCL, this time focusing our attention on the management of early stage disease.
If you have not done so, we highly recommend you listen to our hemepath series before proceeding with this episode. Furthermore, if you have not listened to the introduction to DLBCL episode (Episode 072), we highly recommend doing so, as we will be building on these basics this week.
General reminders from last week:
Fine needle aspiration can be sufficient for diagnosis of solid tumor malignancies and can often be done a lot faster than a core/excisional biopsy, so if differential is broad, can consider starting with FNA.
However, a true diagnosis of lymphoma will require an excision or a core needle biopsy to understand the lymph node architecture
CD10+ indicates that this is likely germinal center origin lymphoma and allows us to formulate an early differential diagnosis. This differential isn’t perfect but can help in more complicated cases. Always think of the following for germinal center origin cases:
Follicular Lymphoma
DLBCL
Burkitt Lymphoma
Flow cytometry:
Increased side scatter = larger cell size
What is the role of the PET/CT in the diagnosis of DLBCL?
PET/CT plays a critical role in helping to distinguish early stage vs. advanced stage disease, which has implications on treatment:
Early stage: A single nodal group, single site of extranodal involvement, or lymph nodes confined to the same side of the diaphragm
Some notes about the PET/CT:
Patients with extranodal disease that isn’t contiguous with nodal involvement are not early stage and are advanced stage.
Another way to think about this is that the extranodal disease must be encompassed in the same radiation field as the nodal disease to be considered early stage
In early stage disease, if someone has extranodal disease, we denote it with the letter “E”
This includes marrow, skin, bones, or other solid organs but not the spleen which is considered a nodal structure
Another important distinction is the concept of “bulky” disease. The reason for this is because those with bulky disease are treated similarly to those with advanced disease.
In DLBCL, there are varying definitions but think > 10 cm though some argue this should be > 7.5 cm based on inclusion criteria for a few trials that we will discuss.
Advanced stage disease is defined by either:
Stage III - nodes above and below the diaphragm (spleen is considered a lymph node). Bone marrow is extranodal and would upstage to stage IV.
Stage IV - diffuse involvement of one or more extranodal tissues. Key is that all sites of lymphoma can’t be encompassed in one radiation field. Very similar to limited stage vs. extensive stage small cell lung cancer. Always remind patients that stage IV disease in lymphoma is still curative
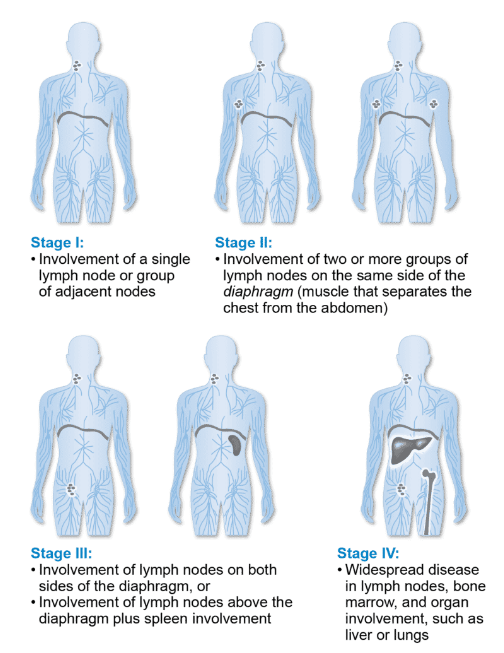
Image source: https://lymphoma.org/understanding-lymphoma/diagnosing-lymphoma/staging-and-prognosis/
How do we interpret the “Deauville score”?
The “Deauville score” also known as the 5 point scale was developed at a workshop in Deauville, France in 2009.
Developed criteria to help with de-escalation of therapy in Hodgkin lymphoma
Radiologists assign a score from 1-5 and compare the uptake of the tracer in the tissue of interest to the mediastinal blood pool and liver.
For DLBCL, a score of ≤3 means that the uptake in the area of interest is equal to or less than that of the liver, which in DLBCL is a complete response
When thinking about initial staging, the score isn’t really that important and plays more of a role in assessing response to treatment.
Generally score of 4 or higher is considered active lymphoma
If the bone marrow is avid AND the patient has not received either G-CSF or chemotherapy recently, this suggests marrow involvement.
In this case, we upstage the patient and assume they have marrow involvement (no marrow is needed because it won’t change management)
Patients with early stage disease will very rarely have marrow involvement and so almost always, bone marrow biopsy is not needed
What are other important aspects of the pathology report?
FISH report to establish if patient has MYC +/- BCL-2 +/- BCL-6 rearrangements
Note: additional copies is not a rearrangement and plays a minor role
Refer back to episode 072 for a further discussion about this
Finally: remember to calculate the patient’s IPI score (also discussed in episode 072)
In early stage DLBCL, how do we approach treatment?
Some historical context:
For decades, starting in the 1970’s the historical standard of care treatment in DLBCL was CHOP chemotherapy
Included cyclophosphamide, doxorubicin (previously called hydroxydaunorubicin hence the H), vincristine (also known as oncovin hence the O), and prednisone
CHOP chemotherapy including cyclophosphamide, doxorubicin, vincristine, and prednisone was the standard of care until 2002 when there was a trial that showed OS benefit of R-CHOP vs. CHOP
In the early era, CHOP and R-CHOP was often given for 8 cycles until we realized that 6 cycles was sufficient
But many researchers knew that we could probably get away with less combination chemotherapy for early stage disease
There were prospective studies done in the 1980’s that suggested 3 cycles of CHOP followed by RT had similar outcomes to 8 cycles of CHOP of early stage DLBCL
This concept became the conceptual framework for how we treat these patients today
The first pivotal randomized trial in early stage DLBCL was done by the SWOG cooperative group published in NEJM 1998, called S8736
Included early stage patients without bulky disease
Randomized patients to CHOP x 8 cycles vs. CHOP x 3 cycles followed by IFRT (involved field radiotherapy)
5 year OS improved to 82% from 72% favoring CHOP x 3 followed by IFRT so a 10% absolute gain in OS
This was also a less toxic regimen and became a reasonable standard of care for early stage disease
Interestingly, long term follow up published in JCO 2016 showed no difference in PFS or OS with median follow up of nearly 18 years
Nonetheless, we are sparing patients additional cycles of chemotherapy
There was then a phase II study that looked at R-CHOP x 3 followed by IFRT by the SWOG group called S0014 (***Note here that they included the “R” AKA rituximab to the CHOP backbone)
Included early stage patients without bulky disease
The data suggested that administering 3 cycles of R-CHOP followed by radiation improved PFS and OS if you do a cross trial comparison to CHOPx3 therapy
Not a perfect analysis but did improve OS by another 5-10%
This then became a reasonable choice for treatment of early stage patients and could be offered to our patient in this case
Are there options that do not use radiation?
R-CHOP x 4
If pursuing this option, patients must get an interim PET/CT after 3 cycles of R-CHOP and if they are in CR, then they can proceed to their final cycle of R-CHOP
How did we come up with this strategy?
We actually learned about this when there from a single arm phase II trial that evaluated the use of a novel drug called ibritumumomab tiuxetan (Y90 CD20 Antibody) that was never approved
In this study, early stage patients without bulky disease were given R-CHOP x 3 and then stratified based on interim PET results
If in CR, then the patients got one more cycle of R-CHOP
If in PR, then the patients got IFRT + this new therapy
Let’s focus on those in CR
The 5 year OS was 91% which is concordant with the data observed with R-CHOP x 3 followed by IFRT in that phase II SWOG trial we discussed
This is why R-CHOP x 4 is a reasonable standard of care for early stage patients and can avoid the late toxicity of radiation therapy
The last trial we need to discuss for early stage patients is a phase III non inferiority randomized trial called the FLYER study
Here we looked at the most favorable patients
Early stage, non bulky (defined by 7.5 cm) and an IPI of 0
Randomized to R-CHOP x 4 followed by single agent R x 2 cycles vs. R-CHOP x 6 cycles
No difference in PFS or OS with long term OS ~98%
Technically this is an option for R-CHOP x 4 followed by 2 cycles of R but this is likely over treatment as R-CHOP x 4 should be sufficient
What if your patient has early stage DLBCL but FISH results suggest they have high grade B-cell lymphoma (double or triple hit)? Do we escalate therapy to a more intensive regimen?
Limited data in this space, but one good retrospective study that showed there is no difference in outcomes when using the standard approaches vs. intensive combination chemotherapy like DA-REPOCH for early stage patients
Typically, we would not recommend escalating therapy in early stage disease in the absence of high burden of disease, such as a large mediastinal mass or bulky adenopathy
What is the approach for older patients with early stage DLBCL?
For patients older than 80 (or more frail): dose-reduced R-CHOP AKA R-miniCHOP
For patients younger than 80: R-CHOP with G-CSF support
For patients who cannot tolerate an an anthracycline: R-miniCEOP or R-GemOx are reasonable options
For patients with poor performance status: Start with “pre-phase” treatment meaning the giving prednisone 100 mg daily x 5-7 days prior to starting therapy can help you assess how much of their performance status decrement is related to disease vs. baseline function
We often see an improvement in performance status relatively quickly with prephase steroids and you will see that older studies from Germany included 1 mg of vincristine with the steroids but that is likely not necessary
References
https://ascopubs.org/doi/full/10.1200/JCO.2013.54.8800 Article on Lugano Staging and response criteria
https://ascopubs.org/doi/abs/10.1200/JCO.1989.7.9.1186?role=tab: JCO article suggested 3 cycles of CHOP followed by RT had similar outcomes to 8 cycles of CHOP of early stage DLBCL
https://www.nejm.org/doi/full/10.1056/NEJM199807023390104 : S8736 study comparing CHOP x8 cycles vs. CHOP x3 cycles + IFRT
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5012710/ : Long term follow up data on S8736 study
https://pubmed.ncbi.nlm.nih.gov/18413640/ : S0014 study investigating R-CHOPx3+IFRT
https://www.thelancet.com/article/S0140-6736(19)33008-9/fulltext : FLYER study showing non-inferiority of R-CHOP x4 + 2 cycles of Rituximab compared to 6 cycles of R-CHOP
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6988401/ : Retrospective analysis investigating DA-R-EPOCH for early stage patients with high risk features on FISH
https://ashpublications.org/blood/article/116/24/5103/28024/How-I-treat-elderly-patients-with-diffuse-large-B : ASH “How I Treat” article for DLBCL in elderly patients
The crew behind the magic:
Show outline: Vivek Patel
Production and hosts: Ronak Mistry, Vivek Patel, Dan Hausrath
Editing: Resonate Recordings
Shownotes: Ronak Mistry
Social media management: Ronak Mistry

We are proud to partner with HemOnc.org!
Want to learn more about the trials that lead to the regimens discussed today? What about dosing schedules? See links in the show notes for a link to HemOnc.org