
Episode 024: Lung Cancer Series, Pt. 2: Fundamentals of histology and staging
Lung cancer is one of the most commonly diagnosed type of cancer and so it is fitting that we start the first of our disease-specific oncology series with this diagnosis. This week, we go through the fundamentals of histology and staging.
If you have not done so, we highly recommend you listen to last week’s episode first!
Lung Cancer Histology and Staging
Workup for a nodule that is concerning:
Ensure there is a dedicated CT scan of the chest to evaluate
Try to obtain old imaging; the rate of change is important
Can get PET, but even if a lesion if not FDG-avid, but growing quickly we should consider biopsy anyway
Referral to pulmonary medicine, who can assist with biopsy and also regional lymph node evaluation (important – more below)
PFTs are often ordered because it provides information about lung function in anticipation of possible surgery for treatment
Lung Cancer Histology:
Non-small cell lung cancer (NSCLC)
Umbrella term for a variety of cancers
Increased risk in smokers
More common types:
Adenocarcinoma (~50% of all lung cancers)
Most common overall; cancer of the mucus producing cells
IHC: TTF-1, NapsinA, CK7 positive
Squamous Cell Carcinoma (22.7%)
More often seen in patients with a smoking history
IHC: p63 positive and cytokeratin pearls
Remaining ~15% are the other types of lung cancer / mixed histologies
Small cell lung cancer (SCLC)
Neuroendocrine tumor with very different pathology
Much more aggressive than NSCLC
Oncologic emergency
IHC: Chromogranin and synaptophysin positive
IHC pearls: TTF-1 usually means lung cancer (but can be negative in squamous cell lung cancer). This will be important in the future (we promise :])
Staging for NSCLC:
Nodal evaluation: lymph node evaluation is part of the workup for NSCLC
Single digit = central/mediastinal nodes (higher risk)
Double digit = peripheral/hilar/intrapulmonary lymph nodes (lower risk)
“R” vs. “L” is direction
Pearl: Why is this important? If there is nodal involvement, systemic therapy is going to be necessary
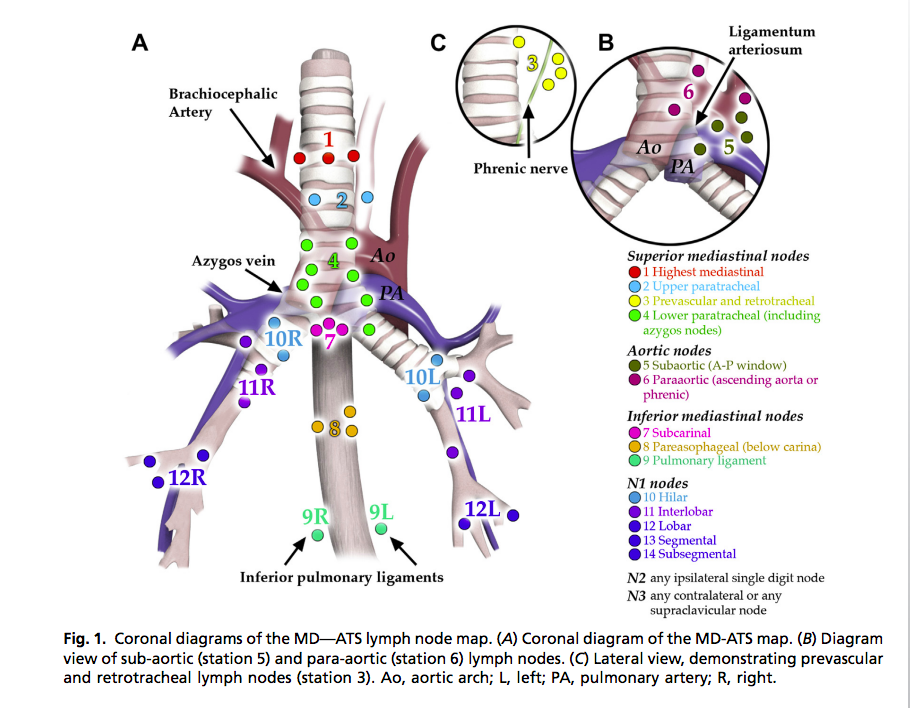
Nodal stations. Image source: http://dx.doi.org/10.1016/j.ccm.2013.04.008
Putting it all together:
T: Tumor size
T1-4
N: Nodal involvement
N0: no nodal involvement
N1: Nodes closest to the primary tumor (double digits)
Ipsilateral peribronchial, hilar, intrapulmonary
N2: Further away (single digit)
Ipsilateral mediastinal and/or subcarinal LN
N3: Contralateral any node or supraclavicular LN
M: Metastasis – in lung cancer, patients with certain patterns of metastatic disease are still curable!
M0: no mets
M1a: Contralateral lobe, pleural effusion or pericardial effusion à these are generally still curable!
M1b: single site of metastatic disease à these are generally still curable!
M1c: multiple sites of metastatic disease à these are generally not curable
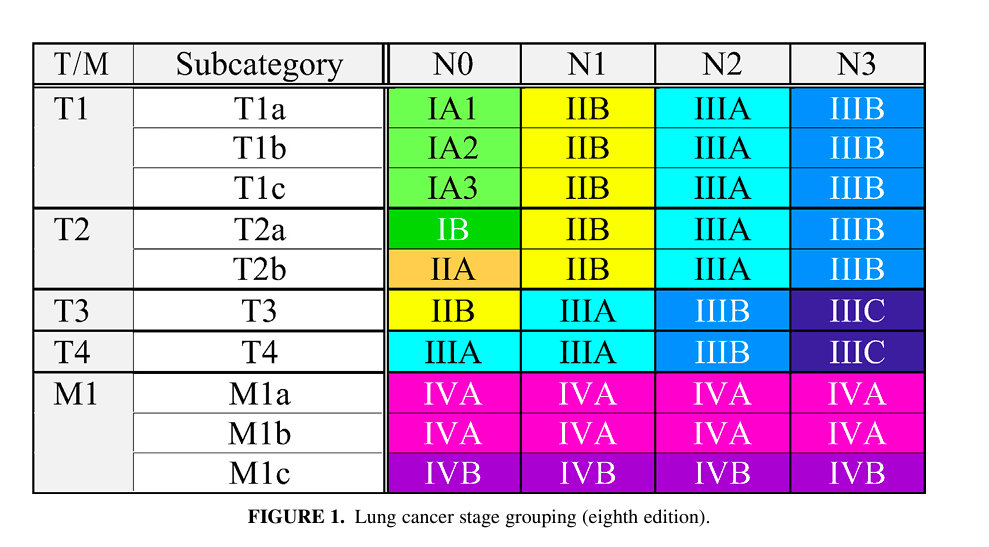
Staging for lung cancer. Image Source: https://doi.org/10.1016/j.jtcvs.2017.08.138
Staging for SCLC:
Limited stage - meaning it can fit in “one radiation field”
Extensive stage - does not fit in “one radiation field”
Once lung cancer is diagnosed:
Go to NCCN to learn the flow of ongoing management
Complete staging (if not already done):
CT C/A/P (don’t necessarily need if a PET scan is done)
PET Scan
MRI brain à in general this is needed, but there are some exception to this (see NCCN)
Referral to pulmonary for nodal evaluation
References:
NCCN.org
https://doi-org.proxy.library.vanderbilt.edu/10.1016/j.semcancer.2017.11.019-Article about IHC markers for lung cancer