
Episode 095: Introduction to CLL/SLL
This week, we start a new series, this time all about the ins-and-outs of chronic lymphocytic leukemia (CLL) / small lymphocytic lymphoma (SLL)! Whether practicing general internal medicine, hospital medicine, or hematology/oncology, you will likely come across a patient with CLL. First, we go through initial diagnosis of this disease!
Are smudge cells pathognomonic for chronic lymphocytic leukemia (CLL)?
A smudge cell is a remnant of a lymphocyte that has been smudged (“smushed”) and all that can be seen are remnants of the nucleus
These cells are large and fragile and are prone to being damaged and destroyed during slide preparation
This does not exclusively occur with CLL but can also be seen in viral infections, significant stress due to severe illness, or anything that produces reactive lymphocytes which can be large and fragile
Bottom line: A smudge cell here and there does not necessarily mean the patient has CLL (although a full field of smudge cells is certainly very suspicious)
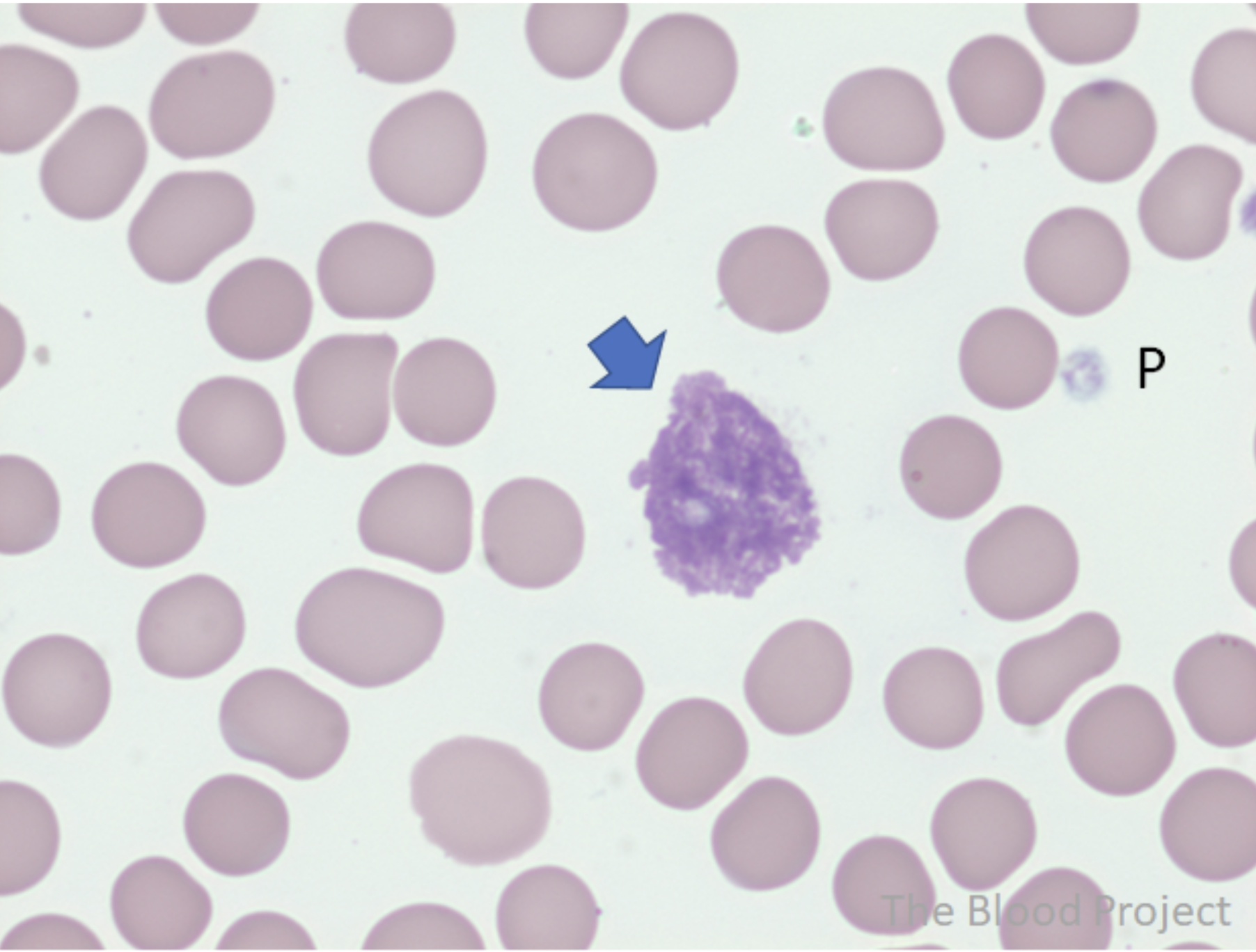
Image source: Image courtesy of The Blood Project by Dr. William Aird (https://www.thebloodproject.com/) No copyright infringement intended.
What is the differential diagnosis of lymphocytosis?
There are multiple etiologies for lymphocytosis including infection (for example, EBV infection / infectious mononucleosis), drug hypersensitivity like DRESS syndrome, asplenia, thymoma, and B cell malignancy
Absolute lymphocyte count (ALC) is very important. Infection can result in lymphocyte counts in the 20-30 K range for some patients, while other causes are often lower, in the 5-15 K range
Maintain a high suspicion for hematologic malignancy if the ALC is above 30 K
How does flow cytometry help in the workup of lymphocytosis?
Flow cytometry is a critical test to help establish clonality and determine whether the lymphocytes are from a single lineage
Hematologic malignancies are characterized by abnormal expression of surface markers and/or aberrant absence of surface markers
Refer back to Episode 002 where we discuss the logistics and applications of flow cytometry
What CD markers help narrow the differential diagnosis of B cell malignancies?
CD5 positive and CD10 negative should make you think of either mantle cell lymphoma (indolent, leukemic variant) or CLL
CD19 bright, CD20 dim, and CD200 bright are very consistent with CLL
CD200 bright is not consistent with mantle cell lymphoma
Mnemonic: CD5 is small and CLL/SLL has small lymphocytic lymphoma in the name, and CD200 bright is long so chronic (i.e. long!) lymphocytic leukemia is likely
Correlation with the morphology of these cells is also important, so read the full pathology report
Why is this diagnosis called chronic lymphocytic leukemia / small lymphocytic lymphoma?
Leukemia is generally defined by circulating malignant cells from the hematopoietic lineage in the peripheral blood. For example, there can be a leukemic phase of diffuse large B cell lymphoma if there are circulating large lymphoma cells in circulation
What makes a diagnosis of CLL?
Absolute lymphocyte count > 5000
Immunophenotype consistent with CLL on flow cytometry
What is the pathogenesis of CLL?
B cells originate from the marrow from CD34+ progenitor stem cells
As the B cell matures, it will eventually circulate in the peripheral blood to look for a lymphoid organ to live in (like a lymph node or the spleen)
The naïve B cell enters a lymph node to undergo further maturation. There, it will get exposed to an antigen and undergo somatic hypermutation of the immunoglobulin heavy chain in the germinal center of the lymph node
The malignant clone for CLL can either be the naïve B cell or the more mature B cell that has undergone mutation of the immunoglobulin heavy chain
In either case, these B cells are freely circulating in the peripheral blood and taking up residence in the lymph nodes - depending on the dominant behavior of the cell when it developed a malignant clone, it can be more predominant in the blood (where it is diagnosed as CLL via flow cytometry) or more in the lymph nodes (where it is diagnosed as SLL via a lymph node biopsy)
Either way it is the same exact malignant clone, and typically cells will be found in both the blood or lymph node. Most patients have higher circulating CLL cells than malignant cells residing in lymph nodes. However, some patients have more lymph node predominance and will be diagnosed with SLL.
What is the natural history of CLL?
CLL is not like other “leukemia” diagnoses so it is important to explain this distinction to the patient!
This is the most common type of leukemia accounting for ~ 1% of all new cancer diagnoses in the US
It most commonly occurs in older patients with a median age of diagnosis of 70
There are some patients who will never need treatment, but the majority of patients will need treatment at some point but often have good long term survival
However, there are a subset of patients who follow a more aggressive disease course - so it is important to risk stratify and monitor higher risk patients closely
How do patients with CLL progression typically present?
B cells secrete autoantibodies. These autoantibodies can cause autoimmune cytopenias in some patients, which is usually an indication to treat
Other patients will have autoimmune conditions due to autoantibody production from their CLL clones
Still other patients will simply have B symptoms due to low level cytokine storm, such as fever, weight loss, night sweats, splenomegaly, bulky lymphadenopathy, early satiety, and fatigue
Do all patients need imaging and/or a bone marrow biopsy?
You can get a great deal of information from peripheral blood testing. Therefore, a bone marrow biopsy is often not needed for patients with CLL given the abundance of circulating malignant cells (see more below!)
Imaging is not necessarily required for patients who are asymptomatic
A thorough lymph node exam at the time of diagnosis is very helpful
What are the two (older) staging systems for CLL?
Rai stage and Binet stage
What is the Rai staging system?
The Rai stage was developed in 1975
The study looked at 125 patients diagnosed from 1941 to 1971. The authors chose somewhat arbitrary (!) staging cutoffs based on clinical experience and prior retrospective data and tested applicability overall survival by validating the stages with this cohort and two other retrospective datasets
Stage 0 was lymphocytosis only
Stage 1 was lymphocytosis with lymphadenopathy
Stage 2 was hepatomegaly or splenomegaly
Stage 3 was anemia, defined by hemoglobin less than 11 g/dL
Stage 4 was thrombocytopenia defined by platelet count less than 100 K
These stages should not be used for prognostication in the modern era, as this system was developed based on patients from the 40s through 70s!
Stage 0 patients had median overall survival well over 10 years, which confirms that these patients can have a very indolent course

Rai Staging
What is the Binet staging system?
The second system is the Binet stage, done by a French group
The original publication in 1977 had a 4 stage system very similar to Rai with slight differences:
No stage 0
Stage 1 patients had lymphadenopathy and lymphocytosis
Splenomegaly was used for stage 2 and 3
Stage 4 was either anemia or thrombocytopenia
Then, in 1981, Binet found that neither Rai staging nor Binet staging was well validated in multivariate models (for example, patients with Stage 0, 1 and 2 all did the same, as did Stage 3 and Stage 4 patients)
Binet then further refined to stages A, B, and C
Using a stepwise selection approach, they found that any cytopenia identified the highest risk patients, which they called Stage C for cytopenias
They then found a correlation with lymph node site involvement for patients without cytopenias counting the spleen as a nodal site. A relatively arbitrary cutoff of 3+ nodal areas vs. < 3 involved nodal areas involved was chosen for prognostication
A: Lymphocytosis with fewer than 3 nodal areas involved
B: Lymphocytosis with 3 or more nodal areas involved
C: Cytopenias (Hgb < 10 or Plt < 100)

Binet staging.
What is the role of IGHV mutation evaluation?
An important study in 1999 utilized a molecular test evaluating the immunoglobulin heavy chain variable region (IGHV)
They looked at about 85 patients and utilized peripheral blood molecular testing to identify patients with CLL cells with mutated IGHV compared to germline homology vs. unmutated IGHV
The hypothesis was that naïve B cells would not have gone through the germinal center and would have unmutated IGHV, whereas more mature B cells would have undergone somatic hypermutation and have a mutated IGHV compared to germline
There was a clear difference in overall survival favoring patients with mutated IGHV (more mature B cells) compared to unmutated IGHV
But at that time, widespread applicability was quite difficult due to logistical difficulties with molecular studies.
A surrogate flow cytometry marker evaluating ZAP-70 expression was developed
This was also a difficult test to run! ZAP-70 is expressed on many cells and you would have to isolate expression in just the CLL cells.
ZAP-70 expression was associated with a worse prognosis
Nowadays we don’t use ZAP-70, given widespread ability to obtain IGHV mutation status
You might also see CD38 expression as a prognostic marker - this is also now outdated
Bottom line: Patients with mutated IGHV have a much better prognosis than patients with unmutated IGHV. (In fact, there may be a subset of patients with mutated IGHV that may be curable!)
What is the role of FISH testing?
There was a pivotal study published in NEJM in 2000
The authors looked at 325 consecutive patients with CLL and ran peripheral blood FISH testing to identify prognostic cytogenetic abnormalities
The most common was deletion 13q which had the most favorable prognosis as the sole abnormality
Deletion 17p had (by far) the worst prognosis
Remember that 17p is the location for TP53 mutations which explains the poor prognosis and general chemo-refractory nature of these patients
Deletion 11q was an intermediate adverse prognostic marker - not as bad as del17p
Deletion 11q seemed to have an adverse prognosis mainly for younger patients below age 55
Everything else: trisomy 12, no changes, and deletion 7q didn’t matter quite as much
They did tend to have a good prognosis overall
Keep in mind that these patients were all treated in the chemotherapy era, prior to modern therapies like BTK inhibitors and venetoclax

What is the role of CLL-IPI in risk stratification?
As with the other systems, the CLL-IPI score is also outdated in terms of overall survival, as it was developed prior to modern therapies like BTK inhibitors and venetoclax
There were two large efforts to identify an appropriate risk score in CLL (like IPI in large cell lymphoma)
One was from the German CLL Study Group (GCLLSG):
This incorporated several variables (age, sex, Beta-2-microglobulin, performance status, thymidine kinase, IGHV mutation status, del 11q, and del17p) with del17p as the most heavily weighted factor
Important to know because it was the inclusion criteria for a trial that will be discussed in the next episode which evaluated ibrutinib vs. observation in asymptomatic patients with CLL
The other system, CLL-IPI, was a systematic review and individual patient level meta-analysis published in Lancet Oncology 2016
The primary analysis included patient data from 8 clinical trials. Results were then validated in two separate datasets from the Mayo clinic and a population based Scandinavian cohort. There were nearly 3500 patients included for the primary analysis to develop the CLL-IPI.
There were five independent prognostic markers identified and these were validated in the two other datasets:
TP53 mutation status (either del17p or TP53 mutation on molecular testing)
IGHV mutation status
Serum beta-2 microglobulin (a cutoff of 3.5 mg/L was utilized)
Binet or Rai stage (A vs. B/C for Binet or 0 vs. 1-4 for Rai)
Age (less than or older than 65)
Deletion 11q was not a significant prognostic marker!
As mentioned previously, age seems to be important in patients with deletion 11q
For patients with low risk, over 80% never needed treatment after 10 years of follow up
However, for the other risk groups, overall survival data is unreliable now that there are new highly efficacious therapies available
It is not critical to obtain a beta 2 microglobulin because it will not change management
When might a bone marrow biopsy be indicated?
Some providers obtain a marrow routinely as part of their workup, which isn’t necessarily wrong
However, in most cases, it is not really necessary.
There are some cases where a bone marrow biopsy may be more strongly considered:
Patients with pancytopenia where there is concern for another process like myelodysplastic syndrome
Very symptomatic patients with bulky adenopathy and FDG avid marrow on PET/CT (to rule out potential Richter transformation to large cell lymphoma)
What is the role of imaging?
It is typically helpful to obtain baseline staging imaging
Conventional CT imaging is often sufficient
One advantage of a PET/CT in a patient with CLL who has developed B symptoms is to rule out Richter transformation
Try to biopsy the most FDG avid lymph node
As discussed above, bone marrow biopsy should be performed
Richter transformation has a very poor prognosis, with a 2-year overall survival of under 20%
Many of these patients are referred for allogeneic stem cell transplantation as consolidation therapy
For anyone curious what we were discussing in our intro: What was that Sicilian grape variety again?
Nerello Mascalese
References:
https://www.sciencedirect.com/science/article/pii/S000649712070964X: Rai Staging
https://acsjournals.onlinelibrary.wiley.com/doi/abs/10.1002/1097-0142%28197708%2940%3A2%3C855%3A%3AAID-CNCR2820400239%3E3.0.CO%3B2-1: Original Binet Staging
https://acsjournals.onlinelibrary.wiley.com/doi/10.1002/1097-0142%2819810701%2948%3A1%3C198%3A%3AAID-CNCR2820480131%3E3.0.CO%3B2-V: Updated Binet Staging
https://ashpublications.org/blood/article/94/6/1848/175735/Unmutated-Ig-VH-Genes-Are-Associated-With-a-More: Study evaluating unmutated IGVH
https://www.nejm.org/doi/10.1056/NEJM200012283432602: NEJM Study evaluating prognostic implications of chromosomal changes in CLL
https://ashpublications.org/blood/article/124/1/49/33152/Development-of-a-comprehensive-prognostic-index: CLL Prognostic system developed by German Group
https://www.thelancet.com/journals/lanonc/article/PIIS1470-2045(16)30029-8/abstract: Development of CLL-IPI score
The crew behind the magic:
Show outline: Vivek Patel
Production and hosts: Ronak Mistry, Vivek Patel, Dan Hausrath
Editing: Resonate Recordings
Shownotes: Neil Biswas, Maria Khan
Social media management: Ronak Mistry

We are proud to partner with HemOnc.org!
Want to learn more about the trials that lead to the regimens discussed today? What about dosing schedules? See links in the show notes for a link to HemOnc.org